Atrial Fibrillation
The heart is comprised of 4 chambers; 2 atria, which sit on 2 ventricles. An electrical “timekeeper”, called the sino-atrial node, is located at the top of the right atrium. This is the heart’s natural pacemaker, sending out regular electrical impulses that travel through pathways which run down the atria, through the ‘junction box’ of the heart (known as the AV node) and into the ventricles, allowing the heart to contract and relax regularly and pump blood around the body.
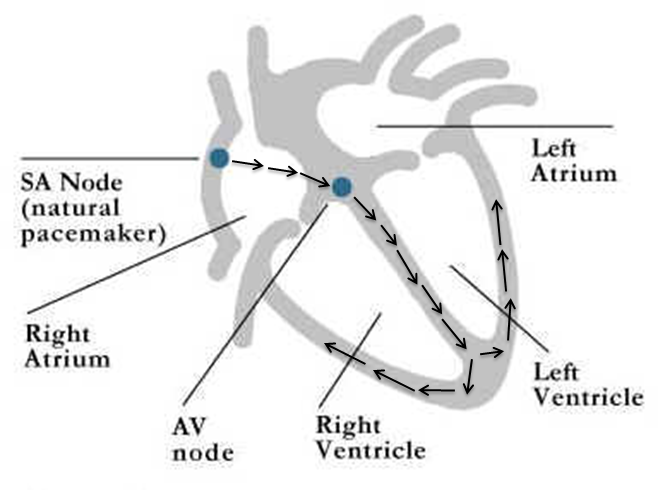
Normal ‘sinus’ rhythm (see text for details)
Sometimes other parts of the atria fire off random electrical impulses which over-ride those of the sino-atrial node, causing the atria and ventricles to only partially contract, in a disorganised way; this is called atrial fibrillation (AF). The heart often beats very fast and irregularly, each beat with variable intensity.

Symptoms of AF commonly include palpitations, shortness of breath, and fatigue. Some patients experience dizziness, chest pain and can occasionally lose consciousness. An ECG (electrocardiogram) and Echo (echocardiogram), both non-invasive tests, are usually sufficient to make the diagnosis. It is also important to investigate AF to determine if there are any underlying causes as some of these can be reversible.
Treatment of AF is aimed at two main things:
1) the reduction of stroke risk that is associated with AF, and
2) the treatment of symptoms or other complications such as heart failure.
Stroke prevention treatment involves assessing each individual and then working out whether they need to take medication to thin their blood. This may be aspirin, warfarin, or even some new drugs that are just becoming available in the UK (such as dabigatran).
Treatment of symptoms can be either with medication, by cardioversion, where an electrical shock is given to try to stimulate the heart’s normal rhythm, occasionally with a pacemaker or with ablation