Supraventricular Tachycardia
The heart is comprised of 4 chambers; 2 atria, which sit on 2 ventricles. An electrical “timekeeper”, called the sino-atrial node, is located at the top of the right atrium. This is the heart’s natural pacemaker, sending out regular electrical impulses that travel through pathways which run down the atria, through the ‘junction box’ of the heart (known as the AV node) and into the ventricles, allowing the heart to contract and relax regularly and pump blood around the body.
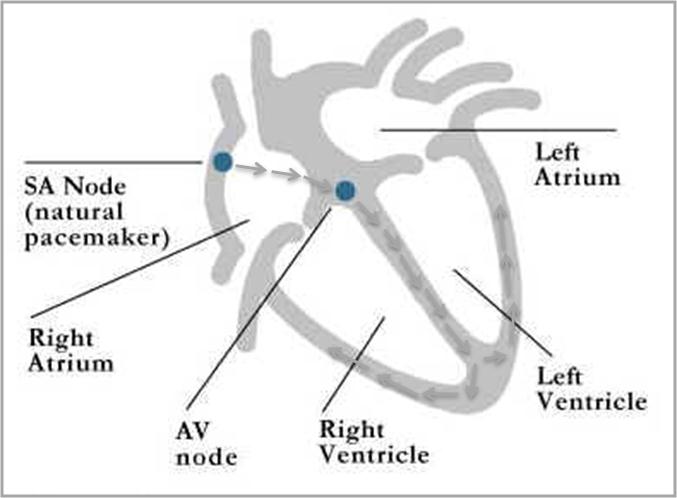
Normal ‘sinus’ rhythm (see text for details)
Supraventricular tachycardia (SVT) simply means that there is a fast heart rhythm that is occurring because of abnormal electrical activity before it reaches the ventricles. These are not normally life threatening but the symptoms can be very debilitating. There are a number of causes, some of which are more common than others. Technically atrial fibrillation and atrial flutter are forms of SVT. However, the most common types of SVT that most people think or are atrioventricular nodal re-entrant tachycardia (AVNRT), atrioventricular re-entrant tachycardia (AVRT) and atrial tachycardia. All three of these can generate abnormal electrical impulses that cause the heart to beat at 140-200 beats per minute or more, in contrast to the normal rate of 60-100 beats per minute. Symptoms can include palpitations, dizziness, breathlessness; in some instances, also chest pain and blackouts.
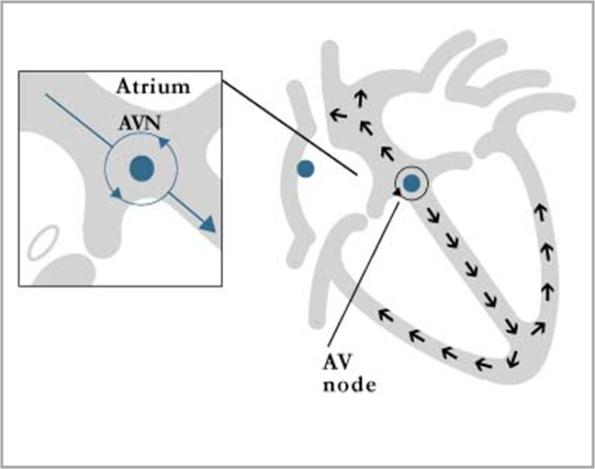
AV nodal re-entrant tachycardia (AVNRT). Many people (30% or more) are born with TWO electrical pathways in the AV node (the junction box of the heart that links the atria to the ventricles labelled AVN in the diagram). Many people will never even know they have two, but some will experience racing of the heart because the signal goes down one pathway but then back up the other, setting up a ‘loop’ of electrical activity that can cause the heart to run at very fast rates. This is a very common type of rhythm disturbance.
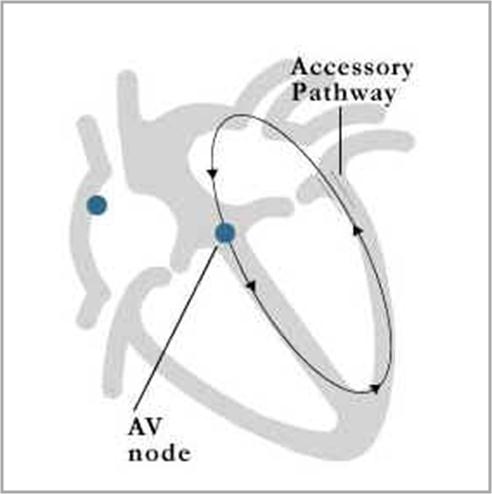
AV re-entrant tachycardia (AVRT). This is not as common as AVNRT. Some people have an extra electrical pathway linking the atria and the ventricles separate to the normal AV node (the junction box of the heart that normally links the atria to the ventricles labelled AVN in the diagram). Many people will never even know they have an extra or ‘accessory’ pathway. In some it can be seen on their ECG Some people will experience racing of the heart because the signal goes down one pathway (usually the normal AV node) but then comes back up the other accessory pathway, setting up a ‘loop’ of electrical activity that can cause the heart to run at very fast rates.
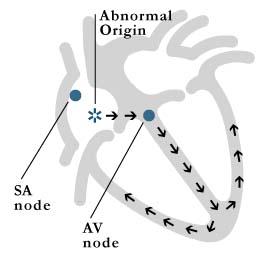
Atrial tachycardia. Unlike AVNRT and AVRT which are abnormal electrical ‘loops’ that occur because of extra electrical pathways in the heart, atrial tachycardia is normally caused by a small bit of tissue (of abnormal origin) in the heart that will intermittently fire off (often very fast) and over-ride the natural pacemaker of the heart (the SA node).
Some people with SVT will identify certain things that set off their palpitations – known as ‘triggers’. Common triggers included caffeine, nicotine, alcohol, stress and exercise, but for many people there is no trigger or pattern and the racing imply occurs anytime, often when sitting doing nothing.
Investigation of SVT is initially by taking a simple ECG. Sometimes ambulatory ECG monitoring is needed, followed by more technical EP studies to try to identify the site of the electrical impulses. Treatment can be with medication but catheter ablation is now increasingly the treatment of choice.